Characteristics
- Most common form of focal dystonia3
- Estimated to affect more than 90,000 people in the United States in 20073
- Misdiagnoses may include tremor, Parkinson’s disease, tics, chorea, psychogenic movement disorder, headache, and scoliosis4

Symptoms5
- Head and neck turning, tilting, or jerking
- Head and neck shaking (spasms)
- Neck and shoulder pain
- Neck and shoulder stiffness
Unlike other forms of focal dystonia, pain is often a prominent symptom with cervical dystonia3
Types of Head Movement
- Torticollis and laterocollis, or a combination of these two, are the most common manifestations5
- Head tremor5

Anterocollis

Retrocollis

Rotational torticollis

Laterocollis
Symptom Stabilization
- Stabilization of symptoms is common but can take several years6
- Remission has been reported in 10% to 23% of patients6
- Progression to segmental dystonia occurs in up to 20% of patients6
Real Patient testimonials
Jan
Jan
Michelle
Michelle
Melissa is a 45-Year-Old ICU Nurse Who Never Backs Down from a Challenge
The life she's fighting for
When she's not running a tight ship at home, Melissa is on the floor of a busy ICU as charge nurse. A leader at heart, Melissa has a passion for life and a personality to match. But nothing makes her prouder than cheering her kids on at their weekly soccer and baseball games.
The weigh-in
- Melissa was diagnosed with cervical dystonia 4 and a half years ago with a posture that includes both torticollis and retrocollis
- She experienced depression and a significant impact in pain
- The pain from cervical dystonia created a challenge in her role as an ICU nurse, which prompted her to seek treatment
Sparring with cervical dystonia
- After years of struggling with pain, Melissa was ready to take control
- She was receiving treatment with a different botulinum toxin for 3 years
- However, after a period of treatment success, Melissa began to suffer a progressive worsening of her cervical dystonia despite increases in dosage

Never defeated, Melissa and her doctor made a change
Explore XEOMIN for the treatment of adult cervical dystonia
Worried about waning efficacy?
Consider XEOMIN
Consider XEOMIN
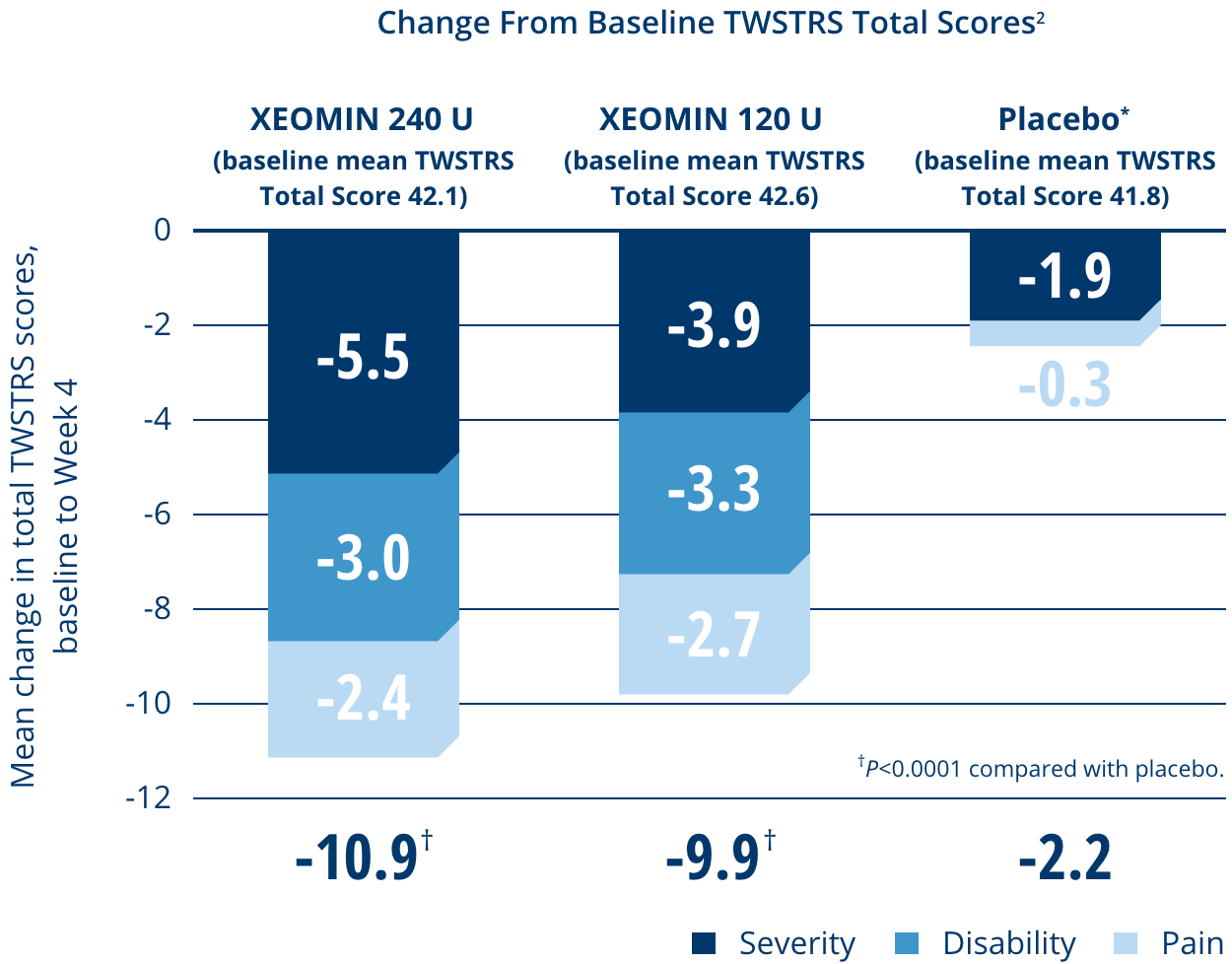
TWSTRS, Toronto Western Spasmodic Torticollis Rating Scale; ICU, Intensive Care Unit.