Causes2-4
- Stroke (most common cause)
- Traumatic brain injury
- Multiple sclerosis
- Spinal cord problems (such as lesions)
- Cerebral palsy in adults

Symptoms4
- Muscle stiffness (known as hypertonia)
- Limited range of movement
- Reduced ability to relax muscles
- Muscle spasms
- Changes in limb position
- Pain
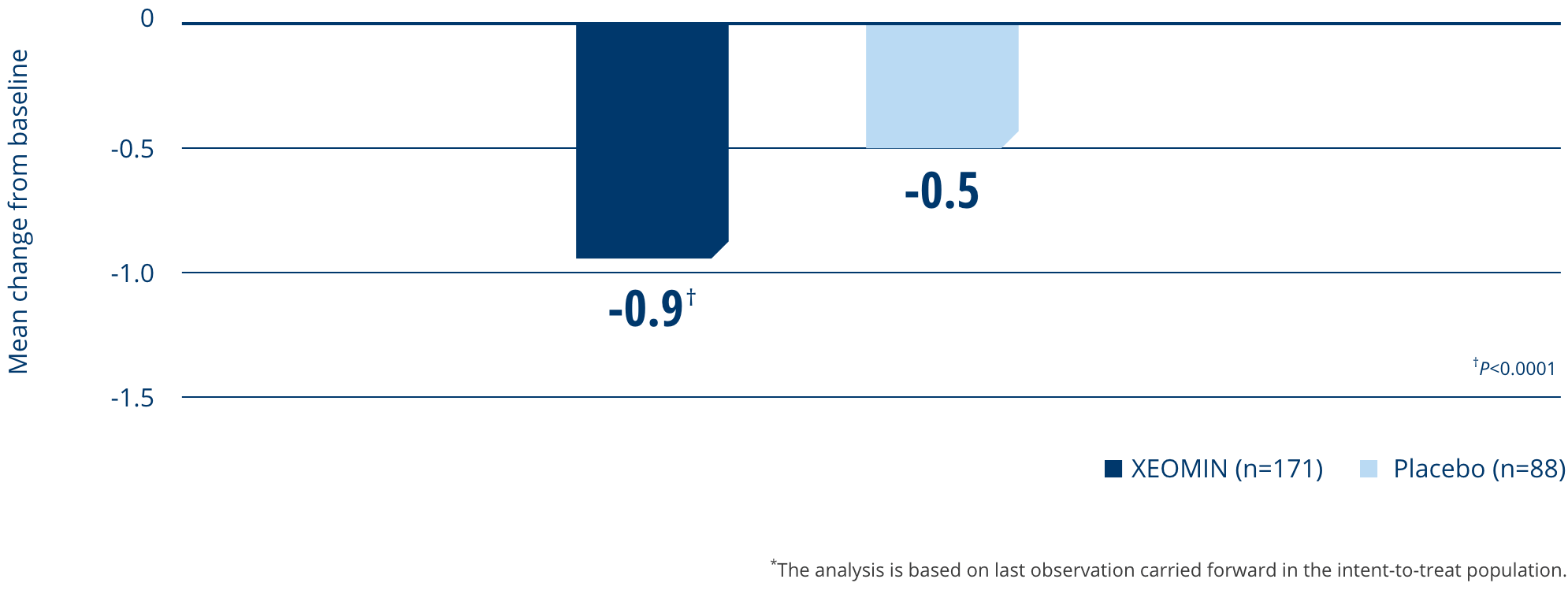
In clinical trials, most patients treated for upper limb spasticity with XEOMIN were adults with
post-stroke spasticity5-7
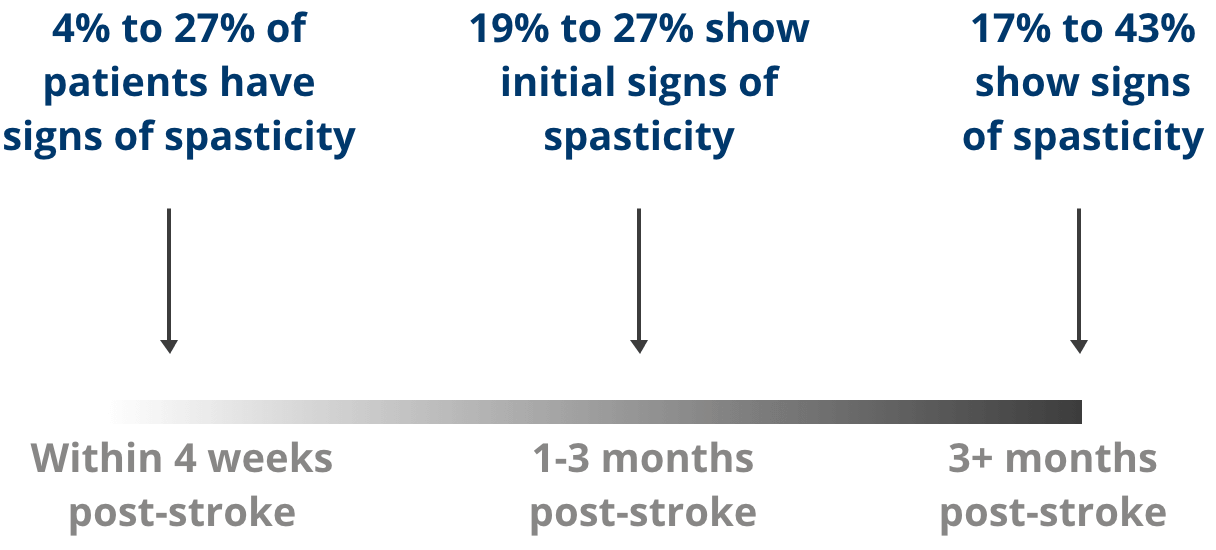
Common Occurrence after Stroke
- Spasticity may be one of many possible consequences after a stroke2
- There is a wide range of prevalence data in post-stroke spasticity, from as little as 19% to as much as 98% of patients8,9
- The onset of spasticity after stroke is also highly variable. It may occur shortly after the stroke or more than 1 year later10
Clinical Patterns

Flexed elbow

Flexed wrist

Pronated forearm

Clenched fist

Thumb-in-palm
Real Patient testimonials
Mike
Russell Is a 61-Year-Old Retired Dentist Who Never Backs Down
The life he's fighting for
After a fulfilling career in dentistry, Russell applied his steady hands to his first love: gardening. His wife, Gabby, an incredible cook, loves his new hobby too, and enjoys incorporating his vegetables into her latest dishes and his flowers into all the rooms of their home.
The weigh-in
- 6 months ago, Russell suffered a stroke; 3 months after that, he began experiencing spasticity in his right arm, which is his dominant arm for performing most of his everyday tasks
- Russell's spasticity is predominantly manifesting in the clinical patterns of flexed wrist, clenched fist, and flexed elbow, which makes it painful and challenging to perform activities like gardening, writing, and cooking in the kitchen with his family
Sparring with upper limb spasticity
- Russell embraced physical therapy, which has helped; however, his range of motion remains limited due to spasticity
- He tried oral medications with limited effect
- Up to this point he has had no prior treatment with neurotoxins

Never defeated, Russell got into the game
Explore XEOMIN for the treatment of upper limb spasticity
Worried about waning efficacy?
Consider XEOMIN
Consider XEOMIN
*Excluding spasticity caused by cerebral palsy.